


PBMs are under fire these days for a lack of transparency about manufacturer rebates and other discounts. But they are trying measures to at least partially shield payers from high MS prices.
This year, Express Scripts launched a programme that reimburses payers for up to half of what they’ve already spent on a DMT if the patient stops taking it within the first three months. The MS programme, which requires the drugs to be filled through Express Scripts’ specialty pharmacy, also provides support for patients during those first few months, including education about potential side effects.
According to the PBM, about a quarter of patients discontinue their medication in the first few months. “If 25% of new patients discontinue therapy, that’s a lot of waste that plan sponsors are paying for that we know doesn’t benefit patients,” says Harold Carter, senior director of clinical solutions at Express Scripts.
This summer, CVS Health announced a programme that would allow any of its payer clients to exclude a newly launched drug – outside of “breakthrough” drugs – that costs more than $100,000 per QALY, according to ICER’s analysis.
Owens questioned whether CVS Health’s move would provide much relief to payers, given that nearly all existing MS drugs far exceed this QALY benchmark. “I don’t think any payer or employer is going to say, ‘Well, these drugs are not cost-effective, so we’re not going to pay for the treatment of MS patients.'”
Economics of adherence
ICER’s analysis also highlighted some gaps in what’s known about DMTs – starting with the limited time frame of clinical trials, typically one to two years. While this trial length is not uncommon, it makes it particularly difficult to assess the benefits and harms of a drug for a disease that progresses over decades, says Dan Ollendorf, ICER’s chief scientific officer.
Ollendorf cites another major knowledge gap: Little research has looked at the optimal sequence for these drugs. For example, he says, “to understand whether patients do better if they start with an interferon and then move on to something more targeted, or vice versa”.
In guidelines released earlier this year, AAN leaders didn’t recommend any specific drugs over others for relapsing-remitting MS. (One exception: They suggested a short list of drugs – Lemtrada [alemtuzumab], Gilenya [fingolimod] and Tysabri [natalizumab] – for patients with signs of highly active MS.) Instead, the expert group provided a consumer-friendly summary of the drugs in alphabetical order, with details of their side effects, method of administration and strength of evidence for relapse prevention.
In contrast, ICER tried to rank the drugs according to their clinical effectiveness. Lemtrada, Tysabri and Ocrevus were identified as most likely to reduce relapses, followed by other drugs based on their relative effectiveness. But will this ICER guidance influence payers’ decisions? At this point, with all the drugs costing roughly the same and no standout options, payers will be more influenced by discounts and rebates in choosing their preferred drug options, says Hartung, the author of the Neurology pricing study.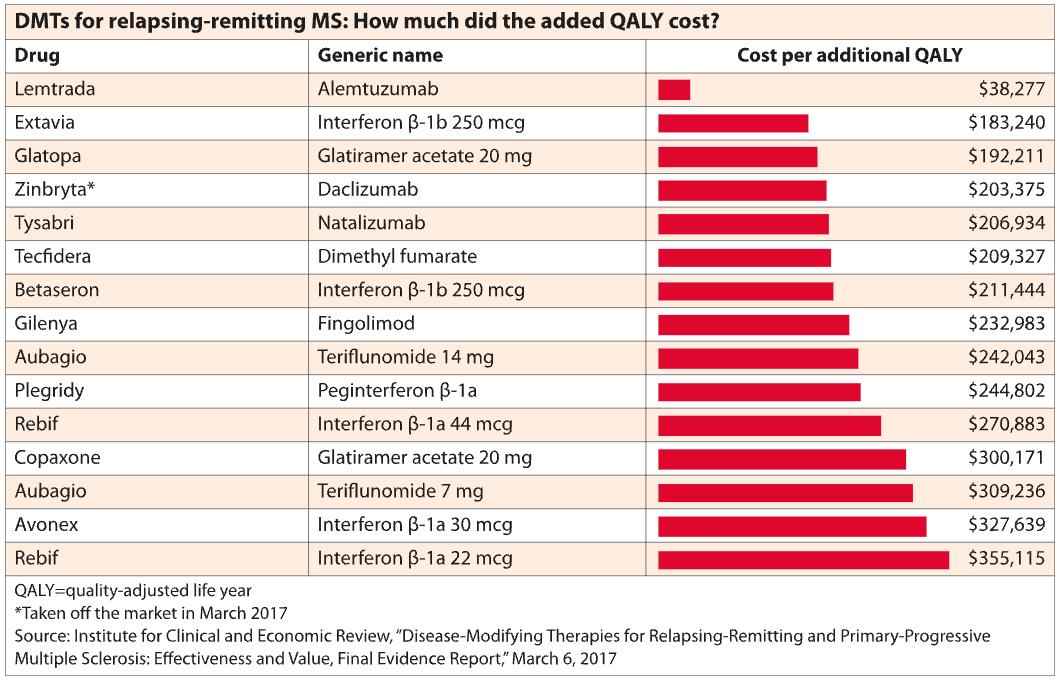 Manufacturers try to make the case that payers will reduce other MS-related costs by spending money on drugs, says Owens. But the reality is that the worsening of the disease, even as disability progresses, is not terribly costly from a payer perspective, he says. A patient might be hospitalised for a short time in the event of a severe relapse. Other expenses include low-cost drugs such as steroids and the purchase of a wheelchair or other medical equipment.
Manufacturers try to make the case that payers will reduce other MS-related costs by spending money on drugs, says Owens. But the reality is that the worsening of the disease, even as disability progresses, is not terribly costly from a payer perspective, he says. A patient might be hospitalised for a short time in the event of a severe relapse. Other expenses include low-cost drugs such as steroids and the purchase of a wheelchair or other medical equipment.
